Research Articles
Association between emotional state and tinnitus severity in a sample of 53 participants
Marta Fernández-Ledesma1 , Ricardo Sanz-Fernández1, María Cuesta2, Pedro Cobo2
, Ricardo Sanz-Fernández1, María Cuesta2, Pedro Cobo2
1 Universidad Europea de Madrid, Tajo s/n, 28670 Villaviciosa de Odón, Madrid, Spain / 2 Instituto de Tecnologías Físicas y de la Información (ITEFI), Consejo Superior de Investigaciones Científicas (CSIC), Serrano 144, 28006 Madrid, Spain.
 OPEN ACCESS
OPEN ACCESS
PEER REVIEWED
ORIGINAL RESEARCH
Abstract
Tinnitus is the perception of sound in the absence of an identifiable internal or external sound source. This symptom affects approximately 14% of the adult population, with prevalence increasing with age. In this study we evaluated the association between emotional state and tinnitus severity in a sample of 53 participants before they started sound therapy. To assess emotional state, the Hospital Anxiety and Depression Scale (HADS) was used, divided into its two subscales for anxiety (HADA) and depression (HADD). To assess tinnitus severity, the Tinnitus Handicap Inventory (THI) and Tinnitus Functional Index (TFI) were used. The sample population showed a strong positive correlation between the HADA and HADD scales and the THI and TFI questionnaires (r = 0.80 and 0.81, respectively). The results corroborate the association between emotional state and tinnitus severity, emphasising the need for an interdisciplinary treatment approach that covers both physical and emotional aspects.
Keywords
Tinnitus, anxiety, depression, THI, TFI, HADS
Clinical implications
Although the qualitative relationship between tinnitus severity (distress) and emotional states is quite well known, the association is rarely quantified through patient studies. Our study quantifies this association by means of the psychometric assessment of tinnitus (THI and TFI) and anxiety and depression (HADS). Understanding our patients’ emotional state may be key when making decisions about the most appropriate type of treatment to reduce tinnitus severity.
Received: 21.09.2023 Reviewed: 09.02.2024 Accepted: 20.04.2024 Published: 24.06.2024
Edited by:
Miriam Isabel Marrufo Pérez
University of Salamanca.
Reviewed by:
Janaina Patricio de Lima
Clínica Universidad de Navarra, Navarra, España.
Byanka Cagnacci Buzo
Cochlear Latinoamérica, Panamá.
An annonymous reviewer
1. Introduction
Tinnitus is defined as the perception of sound in the absence of an internal or external sound source. These symptoms, perceived as ringing or buzzing, are experienced by approximately 14% of the adult population and prevalence increases with age (Jarach et al., 2022). Key risk factors for tinnitus are hearing loss, exposure to noise, age and mental health problems (Johannesen and López-Poveda, 2021; Biswas et al., 2023).
Tinnitus is triggered by abnormal central auditory system compensation for reduced peripheral input (Langguth and Elgoyhen, 2012). Some recent studies suggest that tinnitus can be explained by the decreased neural activity from a damaged cochlea eliciting hyperactivity in the central auditory pathway due to decreased inhibition in the central nervous system (Vasilkov et al., 2023).
Tinnitus has a major impact on a person’s quality of life and well-being because it can lead to problems such as insomnia and stress, and even serious mental health issues (Cobo, 2019). Various studies report that a high proportion of individuals who have tinnitus also have anxiety and depression (Bhatt et al., 2017; Pattyn et al., 2016; Geocze et al., 2013). However, anxiety and depression may not only be comorbidities, but may also be predictors of poor adaptation to tinnitus (Zöger et al., 2006). Møller (2007) suggested that emotional disorders may precede tinnitus and predispose individuals to the onset of this condition.
Anxiety and depression may hinder commitment and adherence to chronic treatments because these emotional states are associated with decreased quality of life and poorer outcomes (Teng et al., 2005; Dickson et al., 2016).
Although the qualitative relationship between tinnitus severity and emotional states is well known, the association is rarely quantified through studies with patients. Therefore, the aim of this study is to identify the strength of the association between emotional state and tinnitus severity. Data offer a means of quantifying the association through psychometric inventories for tinnitus (THI and TFI) and anxiety and depression (HADS). Understanding our patients’ emotional state may be crucial when deciding on the most appropriate type of treatment.
2. Materials and methods
2.1. Subjects
A total of 53 volunteers with tinnitus were recruited through tinnitus associations, advertisements and word of mouth. All volunteers went on to participate in a broader study with personalised sound therapies (Cobo et al., 2021; Cuesta et al., 2022), which is still ongoing. The study was approved by the Research Ethics Committee of the Universidad Europea de Madrid [European University of Madrid]. Participants were excluded if the duration of their tinnitus was less than three months, if they had had recent episodes of vertigo or surgery, had received any previous treatment for tinnitus, or if they had objective tinnitus (caused by a real sound). No specific audiometric criteria were established as an exclusion criterion. All volunteers were given a participant information sheet and signed an informed consent form. They also underwent full audiometric and tinnitus assessments.
Table 1 shows participants’ sex and age expressed as a mean (M), standard deviation (SD), median, maximum and minimum values.
Table 1. Breakdown of participants’ age
|
Total |
Men |
Women |
N (%) |
53 |
36 (68%) |
17 (32%) |
M (years) |
51.7 |
52.0 |
50.9 |
SD (years) |
12.4 |
13.9 |
8.7 |
Median |
51 |
52.5 |
49 |
[Maximum, minimum] |
[78, 24] |
[78, 24] |
[69, 38] |
Table 2 shows the participants’ Pure Tone Average (PTA), covering the frequencies of 500 Hz, 1000 Hz, 2000 Hz and 4000 Hz.
Table 2. Breakdown of participants’ hearing loss
|
Total |
Men |
Women |
PTA RE |
25.47 |
26.49 |
23.30 |
SD RE |
20.09 |
20.69 |
19.18 |
Median RE |
16.25 |
16.25 |
15.0 |
[Maximum, minimum] |
[79, 4] |
[79, 4] |
[76, 4] |
PTA LE |
26.98 |
25.13 |
30.88 |
SD LE |
20.38 |
19.47 |
22.29 |
Median LE |
21.25 |
19.38 |
21.88 |
[Maximum, minimum] |
[87, 4] |
[87, 4] |
[70, 5] |
2.2. Emotional state
To evaluate emotional state, we used the Hospital Anxiety and Depression Scale (HADS) in its Spanish-language version (López-Roig et al., 2000). Study participants completed the online HADS questionnaire prior to starting sound therapy, using a PDF form sent to them by email; the email also contained instructions for completing the questionnaire. The HADS questionnaire was developed in 1983 by Zigmond and Snaith (Zigmond & Snaith, 1983) and was designed for use in clinics and hospital settings. The questionnaire is widely used in research and clinical practice because of its brevity and simplicity, allowing patients to complete it without needing a face-to-face interview. The scale consists of 14 items divided into two subscales for anxiety (HADA) and depression (HADD), which are presented alternately and with responses in varying order. Each item has four response options, scored from "0" (not at all) to "3" (a lot). HADA assesses symptoms of nervousness, restlessness, tension and excessive worry. HADD measures symptoms related to low mood, hopelessness and lack of interest in activities.
The scores for each subscale are scored separately and the total score ranges from 0 to 21 points, from minimum to maximum impact. A score of ≥ 8 on either subscale indicates a clinically significant disorder, and ≥ 11 is considered a moderate-severe disorder.
2.3. Tinnitus severity
Tinnitus severity was evaluated using the Tinnitus Handicap Inventory (THI) and Tinnitus Functional Index (TFI) questionnaires, both in their Spanish versions (Herráiz et al., 2001; Soriano-Reixach et al., 2023). These questionnaires were included in the PDF form with the HADS questionnaire that was sent to participants.
The THI consists of 25 questions and is divided into functional, emotional and catastrophic subscales. Each question has three possible responses, “yes”, “sometimes” and “no”, which are scored with 4, 2 and 0 points, respectively. The total score of all responses ranges from 0 to 100, from minimum to maximum distress. Total THI scores are often used in practice, generally without breakdown by subscale. According to this questionnaire, an individual’s handicap can be classified into one of five categories: 0-16 points, slight handicap; 18-36, mild handicap; 38-56, moderate handicap; 58-76, severe handicap; 78-100, catastrophic handicap.
The TFI, for its part, consists of 25 questions and is divided into eight subscales: intrusiveness, emotions, cognition, auditory difficulties, sleep, quality of life, energy and relaxation. Each of these questions is scored from 0 to 10, where 0 indicates “never” and 10 indicates “always”. The average of all responses is calculated and multiplied by 10 to give a score ranging from 0 to 100 points, for minimum to maximum distress. Like the THI, the TFI score can also be classified into one of five categories: 0%-17%, not a problem; 18%-31%, small problem; 32%-53% moderate problem; 54%-72%, big problem; 73%-100%, very big problem.
2.4. Statistical methods
Pearson's correlation coefficient was used to investigate correlation between the tinnitus (THI, TFI) and emotional variables (HADA, HADD). In order to calculate the degree of significance of these correlation coefficients, the hypothesis test method was applied, where α = 0.05. Therefore, p-values < α indicate statistically significant correlation.
3. Results
We conducted a correlation analysis for emotional state (anxiety and depression), assessed by the HADA and HADD questionnaires, and tinnitus severity measured by the THI and TFI questionnaires.
Table 3 shows the scores for the anxiety (HADA) and depression (HADD) scales in our sample.
Table 3. Breakdown of participants’ emotional state
|
|
Total |
Men |
Women |
HADA |
M |
10.7 |
9.6 |
12.6 |
SD |
4.6 |
4.8 |
3.7 |
|
Median |
11 |
18 |
12 |
|
[Maximum, minimum] |
[20, 2] |
[19, 2] |
[20, 5] |
|
HADD |
M |
8.3 |
7.3 |
10.1 |
SD |
5.3 |
5.4 |
4.2 |
|
Median |
8 |
10 |
7 |
|
[Maximum, minimum] |
[19, 0] |
[19, 0] |
[18, 4] |
The data in the table show the mean (M) and standard deviations (SD), median, and maximum and minimum scores obtained for the anxiety (HADA) and depression (HADD) scales for both sexes, and for men and women separately. In the case of the HADA scale, it is noteworthy that women had a higher mean score for anxiety (12.6) than men (9.6). With regard to the HADD scale, we found that women also had a higher mean score for hospital depression (10.1) than men (7.3). These figures, together with the standard deviations shown in the table, give a detailed picture of disparities by sex in terms of anxiety and depression.
Table 4 shows the average THI and TFI values obtained in our sample.
Table 4. Breakdown of participants’ tinnitus severity
|
|
Total |
Men |
Women |
THI |
M |
55.8 |
52.1 |
63.9 |
SD |
23.9 |
22.6 |
25.3 |
|
Median |
50 |
48 |
68 |
|
[Maximum, minimum] |
[98, 20] |
[90, 20] |
[98, 26] |
|
TFI |
M |
55.6 |
50.5 |
66.4 |
SD |
23.0 |
21.6 |
22.9 |
|
Median |
58.8 |
55.2 |
66 |
|
[Maximum, minimum] |
[99, 10] |
[95, 16] |
[99, 10] |
Table 4 shows the degree of tinnitus-related distress reported via the THI and TFI questionnaires. In the case of the THI, the mean scores were 52.1 and 63.9 for men and women, respectively, indicating a moderate-severe impact of tinnitus on quality of life. Standard deviations were 23.9 and 22.6 for men and women, respectively, indicating variability in the intensity of the perceived handicap. In the case of the TFI, the mean scores were 50.5 and 66.4 for men and women, respectively, indicating a similar perceived tinnitus scores in both sexes. The standard deviations for the TFI were 21.6 for men and 22.9 for women.
Pearson's correlation coefficient (r) was used to identify and evaluate the strength of the relationship between the variables. Correlation factors showed a strong relationship between all anxiety (HADA) and depression (HADD) variables and the THI and TFI scores.
The null hypothesis of no relationship between the variables was tested with a significance level of 0.05. The p-values were less than 10-12, indicating that there is a significant correlation between the tinnitus variables and emotional aspects that we evaluated.
Figure 1 shows the correlation values between the variables evaluated and their degree of statistical significance.
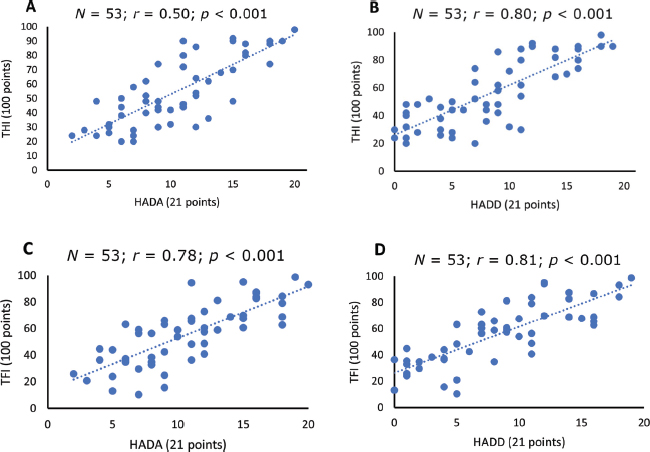
Figure 1. Correlation between tinnitus and emotional variables A) HADA and THI, B) HADD and THI C) HADA and TFI, and D) HADD and TFI.
In addition, the correlation between emotional state (HADA and HADD) and tinnitus severity (THI and TFI) was calculated by separating the data by sex. The results showed a strong correlation in women, although lower than the correlation in men. Table 5 shows the values obtained in our sample.
Table 5. Pearson's correlation coefficient (r) between tinnitus (THI, TFI) and emotional (HADA, HADD) variables in women and men
|
|
THI |
TFI |
Women |
HADA |
0.72 |
0.70 |
HADD |
0.79 |
0.72 |
|
Men |
HADA |
0.82 |
0.79 |
HADD |
0.79 |
0.82 |
4. Discussion
Our study results contribute to the understanding of the relationship between anxiety, depression and tinnitus, three very common symptoms seen in ENT clinics. Numerous research groups have proposed different theories to explain the mechanisms underlying tinnitus (Kaltenbach et al., 2005; Schaette et al., 2006; Eggermont and Tass, 2015). The theory that receives most consensus by the scientific community is based on the neurophysiological model of Jastreboff (1990), regarding the connection between the auditory neural system with the limbic and autonomic nervous systems, responsible for emotions and reactions. These connections provide the background theory of why patients with emotional disorders react more to tinnitus and have a heightened perception of it, which in turn increases distress.
Although most individuals with tinnitus have associated hearing loss, some have normal audiograms (Kara et al., 2020; Tziridis et al., 2021). In these cases, the increased spontaneous activity as a consequence of cochlear synaptopathy is believed to be a feasible explanation of the mechanism causing tinnitus (Schaette and McAlpine, 2011). However, recent research suggests that tinnitus may be due to hyperactivity in the central auditory pathways due to decreased inhibition in the central nervous system (Vasilkov et al., 2023).
From a neurological perspective, anxiety and decreased inhibition are interconnected. Lack of inhibition, which is crucial for proper information processing, may contribute to the onset and persistence of anxiety symptoms. The amygdala and the prefrontal cortex, key areas in emotional response and regulation, play an important role in this relationship. At a neurochemical level, lack of inhibition is associated with imbalances in GABA neurotransmitter signalling, which contribute to increased neuronal excitability and in turn, to anxiety.
The results of our study support these ideas, because we found strong positive correlations between anxiety, depression and perceived tinnitus severity (Cima et al., 2019). The correlation coefficient between the HADA and the two tinnitus questionnaires (THI and TFI) shows a strong positive correlation, with r values of 0.8 in both cases. This finding suggests that as anxiety increases, there is also a significant increase in perceived tinnitus severity (Hackenberg et al., 2023). The p-values for the hypothesis of no correlation are much lower than the significance level of 0.05, indicating that the correlation between the variables is statistically significant. The TFI is more detailed than the THI because it has a wider range of responses (0-10) than the three responses (“yes”, “sometimes” and “no”) in the THI. However, our results are consistent with previous research that has concluded that both questionnaires are valid and sensitive to changes for initial assessments of tinnitus severity (Dehghan et al., 2020; Fernandez et al., 2023).
The absence of significant differences in the correlation values between the questionnaires and emotional state suggests a similar connection in both sexes, although women have higher scores for emotional state and tinnitus severity, and a lower correlation coefficient than men.
There is no consensus in the literature on the prevalence of tinnitus by sex, with some studies suggesting that it is more common in men (Kreuzer et al., 2012; McCormack et al., 2016), while others report no significant differences between men and women (Jarach et al., 2022). Our sample had a higher percentage of men than women (68% and 32%, respectively), although this could be due to the small sample size. However, it is significant that women had higher tinnitus severity scores, as well as anxiety and depression scores across all the questionnaires (+3 in the HADA, +2.8 in the HADD, +11.8 in the THI and +15.9 in the TFI). These findings are consistent with previous studies that have found consistently higher levels of anxiety and depression, and distress in women than men (Seydel et al., 2013; Fioretti et al., 2020). Furthermore, they are in line with the World Health Organization report that acknowledges that women have higher rates of anxiety and depression than men (World Health Organization, 2017). Our study underlines the need to approach tinnitus from an interdisciplinary perspective, taking into account the particularities of each sex, while also considering both clinical and emotional aspects. The interaction between the auditory system and emotional processes highlights the importance of holistic treatment strategies. In this regard, the possibility of strengthening attentional inhibition could also be considered, using non-pharmacological means such as mindfulness practices or selective attention therapies, which may help reduce anxiety and distractions. Some studies confirm that these strategies relieve tinnitus symptoms (Jariengprasert et al., 2022).
In summary, our results corroborate the close relationship between emotional disorders and tinnitus, suggesting the need to carry out interdisciplinary interventions that address both the clinical origin and the emotional aspects alike. Finally, it should be noted that when individual have persisting moderate-severe tinnitus, clinicians are faced with the challenge of investigating whether the anxiety and depressive symptoms are co-morbidities, consequences of the tinnitus, or both.
4.1. Limitations
Limitations of our study include the small sample size, which may have introduced a sex bias. In addition, the participants’ emotional state, including anxiety and depression, was assessed using the HADS questionnaire, without performing a formal psychiatric diagnosis. Furthermore, the study did not investigate whether or not medication was taken for tinnitus. Finally, participants’ hearing loss was not considered in the correlations analysis.
5. Conclusions
The results from our sample of 53 participants highlight the close relationship between emotional state and self-perceived tinnitus severity. We found strong, positive correlations between participants’ anxiety and depression scores, measured using the HADS questionnaire, and their tinnitus severity scores, measured using the THI and TFI questionnaires.
Despite the limitation from the sample’s sex distribution, the consistency of the correlations between tinnitus severity and emotional state suggests a strong association, with a tendency towards higher scores in women.
In summary, this study contributes to our understanding of the complex relationship between the emotional and psychometric aspects of tinnitus, and highlights the need for holistic therapeutic strategies to improve our patients' quality of life.
6. References
Bhatt, J. M., Bhattacharyya, N., & Lin, H. W. (2017). Relationships between tinnitus and the prevalence of anxiety and depression: Tinnitus and Mood Disorders. The Laryngoscope, 127(2), 466–469. https://doi.org/10.1002/lary.26107.
Biswas, R., Genitsaridi, E., Trpchevska, N., Lugo, A., Schlee, W., Cederroth, C. R., Gallus, S., & Hall, D. A. (2023). Low evidence for tinnitus risk factors: A systematic review and meta-analysis. Journal of the Association for Research in Otolaryngology: JARO, 24(1), 81-94. https://doi.org/10.1007/s10162-022-00874-y
Cima, R.F.F., Mazurek, B., Haider, H., Kikidis. D., Lapira A, Noreña. A, Hoare. & D.J. (2019). A multidisciplinary European guideline for tinnitus: diagnostics, assessment, and treatment. HNO, 67, S10-S42.
Cobo, P. (2019). A multidisplinary approach to tinnitus. Loquens, 5(2), 051. https://doi.org/10.3989/loquens.2018.051
Cobo, P., Cuesta, M., & de la Colina, C. (2021). Customised enriched acoustic environment for sound therapy of tinnitus. Acta acustica, 5, 34. European Acoustics Association. https://doi.org/10.1051/aacus/2021028.
Cuesta, M., Garzón, C., & Cobo, P. (2022). Efficacy of sound therapy for tinnitus using an enriched acoustic environment with hearing-loss matched broadband noise. Brain Sciences, 12(1), 82.
Dehghan, M., Fatahi, F., Rouhbakhsh, N., Mahdavi, M. E., Zamiri Abdollahi, F., & Jalaie, S. (2020). The relathinship between tinnitus functional index and tinnitus handicap inventory scores in patients with chronic tinnitus. شنواییشناسی. https://doi.org/10.18502/avr.v29i3.3846
Dickson, J. M., Moberly, N. J., O’Dea, C., & Field, M. (2016). Goal fluency, pessimism and disengagement in depression. PloS One, 11(11), e0166259. https://doi.org/10.1371/journal.pone.0166259
Eggermont, J. J., & Tass, P. A. (2015). Maladaptive neural synchrony in tinnitus: origin and restoration. Frontiers in Neurology, 6, 29. https://doi.org/10.3389/fneur.2015.00029
Fernández, M., Cuesta, M., Sanz, R., Cobo, P. (2023). Comparison of Tinnitus Handicap Inventory and Tinnitus Functional Index as Treatment Outcomes. Audiology Research, 13, 23–31. https://doi.org/10.3390/audiolres13010003.
Fioretti, A., Natalini, E., Riedl, D., Moschen, R., & Eibenstein, A. (2020). Gender comparison of psychological comorbidities in tinnitus patients - results of a cross-sectional study. Frontiers in Neuroscience, 14, 704. https://doi.org/10.3389/fnins.2020.00704
Geocze, L., Mucci, S., Abranches, D. C., Marco, M. A. de, & Penido, N. de O. (2013). Systematic review on the evidences of an association between tinnitus and depression. Brazilian Journal of Otorhinolaryngology, 79(1), 106-111. https://doi.org/10.5935/1808-8694.20130018
Hackenberg, B., Döge, J., O’Brien, K., Bohnert, A., Lackner, K. J., Beutel, M. E., Michal, M., Münzel, T., Wild, P. S., Pfeiffer, N., Schulz, A., Schmidtmann, I., Matthias, C., & Bahr, K. (2023). Tinnitus and its relation to depression, anxiety, and stress-A population-based cohort study. Journal of Clinical Medicine, 12(3). https://doi.org/10.3390/jcm12031169
Herráiz, C., Hernández Calvín, F.J., Plaza, G., Tapia, M.C., & De los Santos, G. (2001). Evaluación de la incapacidad en los pacientes con acúfenos (Evaluation of handicap in tinnitus patients). Acta Otorrinolaringológica Española, 52, 142–145.
Jarach, C. M., Lugo, A., Scala, M., van den Brandt, P. A., Cederroth, C. R., Odone, A., Garavello, W., Schlee, W., Langguth, B., & Gallus, S. (2022). Global prevalence and incidence of tinnitus: A systematic review and meta-analysis. JAMA Neurology, 79(9), 888. https://doi.org/10.1001/jamaneurol.2022.2189.
Jariengprasert, C., Watanapornmongkol, K., Kiatthanabumrung, S., & Wisupagan, T. (2022). The effectiveness of mindfulness-based cognitive therapy in the management of tinnitus. The International Tinnitus Journal, 26(1), 1–10. https://doi.org/10.5935/0946-5448.20220001
Jastreboff, P. J. (1990). Phantom auditory perception (tinnitus): mechanisms of generation and perception. Neuroscience Research, 8(4), 221–254. https://doi.org/10.1016/0168-0102(90)90031-9.
Johannesen, P. T., & Lopez-Poveda, E. A. (2021). Age-related central gain compensation for reduced auditory nerve output for people with normal audiograms, with and without tinnitus. iScience, 24(6), 102658. https://doi.org/10.1016/j.isci.2021.102658
Kaltenbach, J. A., Zhang, J., & Finlayson, P. (2005). Tinnitus as a plastic phenomenon and its possible neural underpinnings in the dorsal cochlear nucleus. Hearing Research, 206(1–2), 200–226. https://doi.org/10.1016/j.heares.2005.02.013
Kara, E., Aydın, K., Akbulut, A. A., Karakol, S. N., Durmaz, S., Yener, H. M., Gözen, E. D., & Kara, H. (2020). Assessment of hidden hearing loss in normal hearing individuals with and without tinnitus. The Journal of International Advanced Otology, 16(1), 87–92. https://doi.org/10.5152/iao.2020.7062
Kreuzer, P. M., Landgrebe, M., Schecklmann, M., Staudinger, S., Langguth, B., & TRI Database Study Group. (2012). Trauma-associated tinnitus: audiological, demographic and clinical characteristics. PloS One, 7(9), e45599. https://doi.org/10.1371/journal.pone.0045599
Langguth, B., & Elgoyhen, A. B. (2012). Current pharmacological treatments for tinnitus. Expert Opinion on Pharmacotherapy, 13(17), 2495–2509. https://doi.org/10.1517/14656566.2012.739608.
López-Roig, S., Terol, M.C., Pastor, M.A., Neipp, M.C., Massutí, B., Rodríguez-Marín, J., Leyda, J.I., Martín-Aragón, M, &Sitges, E. (2000). Ansiedad y depression. Validación de la escala HAD en pacientes oncológicos. Revista de Psicología de la Salud, 12(2), 127-155.
McCormack, A., Edmondson-Jones, M., Somerset, S., & Hall, D. A. (2016). Corrigendum to “A systematic review of the reporting of tinnitus prevalence and severity” [Hear. Res. 337 (2016) 70-79]. Hearing Research, 339, 219. https://doi.org/10.1016/j.heares.2016.08.010
Møller, A. R. (2007). The role of neural plasticity in tinnitus. En Tinnitus: Pathophysiology and Treatment (pp. 37–544). Elsevier.
Pattyn, T., Van Den Eede, F., Vanneste, S., Cassiers, L., Veltman, D. J., Van De Heyning, P., & Sabbe, B. C. G. (2016). Tinnitus and anxiety disorders: A review. Hearing Research, 333, 255–265. https://doi.org/10.1016/j.heares.2015.08.014.
Schaette, R., & Kempter, R. (2006). Development of tinnitus-related neuronal hyperactivity through homeostatic plasticity after hearing loss: a computational model. The European Journal of Neuroscience, 23(11), 3124–3138. https://doi.org/10.1111/j.1460-9568.2006.04774.x
Schaette, R., & McAlpine, D. (2011). Tinnitus with a normal audiogram: physiological evidence for hidden hearing loss and computational model. The Journal of Neuroscience: The Official Journal of the Society for Neuroscience, 31(38), 13452–13457. https://doi.org/10.1523/JNEUROSCI.2156-11.2011
Seydel, C., Haupt, H., Olze, H., Szczepek, A. J., & Mazurek, B. (2013). Gender and chronic tinnitus: differences in tinnitus-related distress depend on age and duration of tinnitus. Ear and Hearing, 34(5), 661–672. https://doi.org/10.1097/AUD.0b013e31828149f2
Soriano-Reixach, M. M., Sampedro, J. J. N., Minguez, M. S. G., Rey-Martínez, J., & Altuna, X. (2023). Translation into Spanish and validation of the Tinnitus Functional Index (TFI). Acta Otorrinolaringologica (English Edition), 74(5), 305–314. https://doi.org/10.1016/j.otoeng.2023.03.003
Teng, C. T., Humes, E. de C., & Demetrio, F. N. (2005). Depressão e comorbidades clínicas. Revista de psiquiatria clinica, 32(3), 149-159. https://doi.org/10.1590/s0101-60832005000300007
Tziridis, K., Forster, J., Buchheidt-Dörfler, I., Krauss, P., Schilling, A., Wendler, O., Sterna, E., & Schulze, H. (2021). Tinnitus development is associated with synaptopathy of inner hair cells in Mongolian gerbils. The European Journal of Neuroscience, 54(3), 4768–4780. https://doi.org/10.1111/ejn.15334
Vasilkov, V., Caswell-Midwinter, B., Zhao, Y. et al. Evidence of cochlear neural degeneration in normal-hearing subjects with tinnitus. Sci Rep 13, 19870 (2023). https://doi.org/10.1038/s41598-023-46741-5
World Health Organization (2017). Depression and other common mental disorders: global health estimates. World Health Organization.
Zigmond, A. S., & Snaith, R. P. (1983). The hospital anxiety and depression scale. Acta Psychiatrica Scandinavica, 67(6), 361–370. https://doi.org/10.1111/j.1600-0447.1983.tb09716.x.
Zöger, S., Svedlund, J., & Holgers, K.-M. (2006). Relationship between tinnitus severity and psychiatric disorders. Psychosomatics, 47(4), 282–288. https://doi.org/10.1176/appi.psy.47.4.282
Acknowledgements
We are grateful for the support provided by the Consejo Superior de Investigaciones Científicas [Spanish National Research Council] (CSIC) and Universidad Europea de Madrid [European University of Madrid].
Author contributions
All authors contributed equally to this work.
Conflict of interest
The authors declare no conflict of interest.
Funds
This research has not received external funding.
Declaration of data availability
The study data are not available due to the confidentiality clause in the informed consent signed by the participants.
How to cite
Fernández Ledesma, M., Sanz, R., Cuesta, M., & Cobo Parra, P. (2024)
Association between emotional state and tinnitus severity in a sample of 53 participants: Emotional state and tinnitus severity. Auditio, 8, e105.
https://doi.org/10.51445/sja.auditio.vol8.2024.105
Correspondence
Marta Fernández Ledesma
C/Tajo s/n, Universidad Europea de Madrid - edificio C, 28670 Villaviciosa de Odón, Madrid, Spain.
Email: marta.fernandez2@universidadeuropea.es
Editorial Office
Copyeditor: Tomás Pérez Pazos
Translation: Emma Goldsmith
Production: Glaux Publicaciones Académicas